
Articulo Original
Fear and anguish: the patient's experience in the intensive care unit
Temor y angustia: experiencia del paciente en la unidad de cuidados intensivos
Medo e angústia: experiência do paciente na unidade de cuidados intensivos
Keydis Sulay Ruidiaz-Gómez1
Shirley Fernández-Aragón2
Abstract
Objective: To understand the experiences of patients who have graduated from the intensive care unit of a tertiary care clinical institution in the City of Cartagena using Rosemarie Rizzo Parse's theory of human development as an approach. Materials and Methods: Phenomenological-interpretive study with a hermeneutic perspective, 11 adults graduated from the intensive care unit participated, the in-depth interview technique was used with a duration of 30 and 40 minutes, the data were analyzed through the technique of intentionality, reduction and constitution. Results: The study participants were eight adult men and three women, their experience was described with feelings of fear and anguish that included the subtopics: Good treatment; Imagination of death: My life, work and family; Feelings of loneliness; Spiritual strength and life changes. Conclusion: Being hospitalized in the intensive care unit managed to trigger an experience described as "fear and anguish", for the participants the family nucleus, spiritual strength, transformation and life changes are essential.
Keywords:Intensive care units; life's experiences; hospitalization; nursing, nursing theory.
Resumen
Objetivo: Comprender las experiencias de pacientes egresados de la unidad de cuidado intensivo de una institución clínica de tercer nivel de atención de la Ciudad de Cartagena utilizando como enfoque la teoría del desarrollo humano de Rosemarie Rizzo Parse. Materiales y Métodos: Estudio fenomenológico - interpretativo con perspectiva Hermenéutica, participaron 11 adultos egresados de la unidad de cuidados intensivos, se utilizó la técnica de entrevista a profundidad con una duración de 30 y 40 minutos, los datos se analizaron a través de la técnica de intencionalidad, reducción y constitución. Resultados: Los participantes del estudio fueron ocho hombres y tres mujeres adultos, su experiencia la describieron con sentimientos de temor y angustia que incluyen los subtemas: Buen trato; imaginación de muerte: Mi vida, el trabajo y la familia; Sentimientos de soledad; Fortaleza espiritual y Cambios de vida. Conclusión: Estar hospitalizado en la unidad de cuidados intensivos logró desencadenar una experiencia descrita como “temor y angustia”, para los participantes es primordial el núcleo familiar, la fortaleza espiritual, la transformación y cambios de vida.
Palabras Clave: Unidades de cuidados intensivos; experiencias de vida; hospitalización; enfermería, teoría de enfermería.
Resumo
Objetivo: Entender as experiências de pacientes formados na unidade de terapia intensiva de uma instituição clínica de terceiro nível na cidade de Cartagena utilizando como foco a teoria do desenvolvimento humano de Rosemarie Rizzo Parse. Materiais e métodos: Estudo fenomenológico - interpretativo com uma perspectiva hermenêutica, participaram 11 adultos formados na unidade de terapia intensiva, foi utilizada a técnica de entrevista em profundidade com duração de 30 e 40 minutos, os dados foram analisados através da técnica de intencionalidade, redução e constituição. Resultados: Os participantes do estudo foram oito homens adultos e três mulheres adultas. Eles descreveram suas experiências com sentimentos de medo e angústia que incluíram os subtópicos: Bom Tratamento; Imaginação da Morte: Minha Vida, Trabalho e Família; Sentimentos de Solidão; Força Espiritual e Mudanças de Vida. Conclusão: Ser hospitalizado na unidade de terapia intensiva conseguiu desencadear uma experiência descrita como “medo e angústia”. Para os participantes, a unidade familiar, a força espiritual, a transformação e as mudanças de vida são primordiais.
Palavras-chave: Unidades de Terapia Intensiva; Hospitalização; Enfermagem, Teoria de Enfermagem.
Introduction
Being hospitalized in an intensive care unit (ICU) generates emotional alterations in the individual such as anxiety, stress, anguish, depression or the so-called intensive care syndrome, this is presented by factors such as excessive noise that hinders sleep, light that It limits rest and the various measures used for ventilation that prevent communication in patients (1-3).
Several authors have dedicated themselves to the study of this problem, in order to know the experiences and feelings present in patients hospitalized in the intensive care unit, Amorós et al. (4), and Beltrán (5-6). They describe the experiences of the patient taking into account that the ICU is an impersonal and technologically invasive environment, its architectural structure favors the loss of privacy, changes in the professional-patient relationship where technology seems to certify the patient's speech, turning the fact into a negative experience; also, it causes suffering in the individual due to the treatment and procedures carried out to resolve the disease (5-7).
The experience of being hospitalized in an ICU is a difficult and painful situation for patients. This generates negative feelings in the person, which significantly mark their life experience, but also trigger positive aspects derived from the humanized care provided by the nursing staff and the renewing experience that generates a significant change for the patient's life, when considering that it is a new opportunity to live again and for a new beginning (8-9).
In accordance with the previous premise, nursing has historically gone from a traditional stage of care to a stage of transformation (10) where it gives value and meaning to the experiences lived by the patient, their environment and family. The constant interaction of the individual with the environment, leads nurses to link different dimensions (social, individual) that influence professional care, to obtain solid elements that help to think about the human being in all its holistic dimension, in addition to creating a new ethical vision aimed at reducing as much as possible the fear, pain and suffering caused by this experience (10-11).
Throughout history, the paradigmatic transformation of nursing as a discipline has been slow and complex. Therefore, the theory of human development proposed by Rosemarie Rizzo Parse (12) is taken as a reference, because it allows structuring the meanings of the human being immersed in a situation, configuring the rhythmic and co-transcendent patterns of the discontinuous situations of the human being, in this case, the experience of being hospitalized in an intensive care unit. The thought of human development articulated with the phenomenological existentialist thought provides the basis for a conceptual system that allows understanding lived experiences, freedom and their participation in life situations, typical of the hermeneutical approach. Likewise, it allows to explore the essence of lived experiences to achieve a deeper understanding of universal human phenomena.
In Cartagena there are few investigations carried out on this individualistic approach, their contributions have been oriented towards coping with and adapting to the disease, therefore, an investigation of this type shows a hermeneutical-transforming vision of care, which leads the nursing professional to use innovative ideas, focused on universal health phenomena and different moments of life, which will contribute to the improvement of nursing practice.
Objective
General Objective
To understand the experiences of adult patients discharged from the intensive care unit of a clinical institution in the City of Cartagena, using Rizzo Parse's theory of human development as an approach.
Materials and methods
A phenomenological-interpretive study was carried out with a hermeneutical perspective according to Heidegger (13-15). The research was developed with the participation of 11 adults who graduated from the ICU, who at the time of the interview were in the hospitalization rooms; who participated in the study voluntarily and without financial or other remuneration from the researchers. With each participant an approach was made and a direct communication was established to publicize the objectives and purposes of the study.
This research implemented an intentional sampling technique (15), mediated by the inclusion criteria: being a patient with an age range between 30 and 80 years (frequent hospitalization population), and having been hospitalized in the ICU for more than 72 hours.
To collect the information, the in-depth interview technique (16) was used, in order to know the experience lived in a phenomenological sense, the dimensions of personal life, the significant experiences, the relationship with the experiences around the subject of interest; in order to be able to search for relationships between global situations and each experience in its particularity.
The first part of the interview was the participant's demographic data, then, in an introductory way, the interview began with the following guiding question: what was the experience lived while you were in the ICU? The interviews were recorded on a magnetic medium (journalism recorder) and completely transcribed in a word processor by the same researcher as soon as the interview was carried out, in order to ensure the information, as it was expressed by the interviewee (17). Each interview was identified with a code and numbered sequentially. The interviews lasted between 30 and 40 minutes approximately, each participant received a total of 2 to 3 interviews in order to deepen the significant experiences.
Once the interview data were collected, they were analyzed according to the Heideggerian perspective, the process includes three stages: intentionality, reduction and constitution. The first, consists of once the interviews are finished, the transcription is carried out, which are compared by reading the text and listening to the audio to confirm the data entered and in this way make a general detail of all the information collected (13). The second involves decision-making by researchers regarding what is main or relevant and what is not. A subtraction is carried out in the transcripts of the interviews, in order to exclude those deviations and sudden changes in the topics and expressions (16,18); Finally, once the information gathering process was finished, a reorganization of the data was carried out, which made it possible to establish connections between the principles of the theory of human development and the phenomena to finally regroup the data (19).
To testify the rigor and quality of the study, the rigorous criteria of qualitative research according to Lincoln and Guba (20-22), credibility, confirmability, applicability and auditability were taken into account, to account for this, each participant was contacted to perform Reading of the initial interviews, the audio recordings and the writings of the interviews were constantly compared with findings contrasted in the literature, the limitations and scope of the research, at the end of the study the final conclusions were shared with the participants and staff from the clinical institution. In addition, the qualitative analysis tool CASPe (23) was used to obtain a critical analysis of the theoretical and internal perspective of the study according to rigor, relevance and credibility. Also, the data were validated through the triangulation of the findings with the literature, the interviews, two experts on the subject and the researcher himself.
Prior to the interview, there was written and verbal authorization from the participants; the interviews, informal conversations and audio notes, transcripts and analysis were stored under security codes in the Drop Box Gmail program in order to protect the anonymity of the participants. To manage the data, pseudonyms and codes were used in each of the interviews in order to safeguard the identity of each participant.
Results
The study participants were eight adult men and three women, with an age range between 32 and 74 years, with complete and incomplete high school and technical and professional training, various occupations, mostly married, of Catholic religion, different socioeconomic strata; with hospitalization in ICU from 5 to 45 days. Among the pathologies that the participants presented for admission to the unit, there were heart failure, chest pain, acute myocardial infarction, head trauma, digestive tract hemorrhages, among others.
The experience can be appreciated from the patients who have graduated from an intensive care unit in Cartagena, where, in light of the principles of the theory of human development proposed by Rizzo (12), the human being is established as a being that constitutes their immersed life experience in an intentional environment where he recognizes his world, acts in the face of adversity and gives meaning to situations, becoming an indivisible being.
The findings showed a central theme where the greatest individual experiences are condensed and six sub-themes related to the principles of the Theory of Human Development (Figure 1). Below are the themes that emerge from the experience:
Central theme: Fear and Anguish
Fear and anguish were considered the feelings expressed by the participants during the time they were hospitalized in the ICU, the patient generates ideas and beliefs as a result of the situation they face. Upon entering the unit they believe that something is not right in their health, so they see death very close, they are unaware of their own illness and everything that happens around them.
Hospitalization in the intensive care unit for the participants became an unknown phenomenon in all areas (personal, family and social), this experience brought with it unexpected experiences, in this context patients become more vulnerable and sensitive to your situation.
Rizzo (12) establishes that the knowledge lived is according to the rhythms expressed by the social patterns of life, here the individual, in this case, the adults graduated from the ICU, create their own experience through uncertainty, sadness and the lack of freedom, therefore, despite having an interdisciplinary team caring for their health, the intensive care unit represents a space where they experience unexpected feelings that generate desperate, fearful and unwanted situations, expressed as follows:
PE2:“Well…., I don't wish that experience on anyone” [….].
PE5:“I was very afraid, very afraid, I felt anguish. honestly ... very, very afraid, very afraid ”. [….].
PE8::“[….] The fear I had because the truth is that I had many crises […]”. [….].
Another sentiment expressed by the adults who graduated from the ICU was despair, an emotion associated with isolation, loneliness and fear; despair arises from the uncertainty of their situation and the fear of being able to die. Many times those who are immersed in despair live life in an anguished way, this was manifested in the following descriptors.
PE2:“Well…., I don't wish that experience on anyone” [….].
PE3: “[…] it's chaotic, desperate […]” "I was going into despair ... the hours were getting long"
PE10:“[…] a lot of uncertainty and concern”. [….].
The participants revealed that they imagined the ICU space very different before entering it; their hospitalization experience was considered hard and heavy. Rizzo's thoughts (8) affirm that the assimilation of the environment is given by contextually constructed liberation, where the human being possesses the ability to perceive and interpret situations in search of an indivisible human universe of constant changes, which unifies his experience to through relationships with the environment.
being has when receiving stimuli from the outside, leads him to make judgments about what surrounds him, be it places, places, noises, sounds, among others. In this regard, they noted:
PE7::“ufff… I imagined that that was something terrible, because one does not imagine it differently”. [….].
PE9:“[…] the hospitalization gave me hard, that environment day and night, horrible […]”.
PE11: "The environment is heavy, very difficult, especially the light and noise."
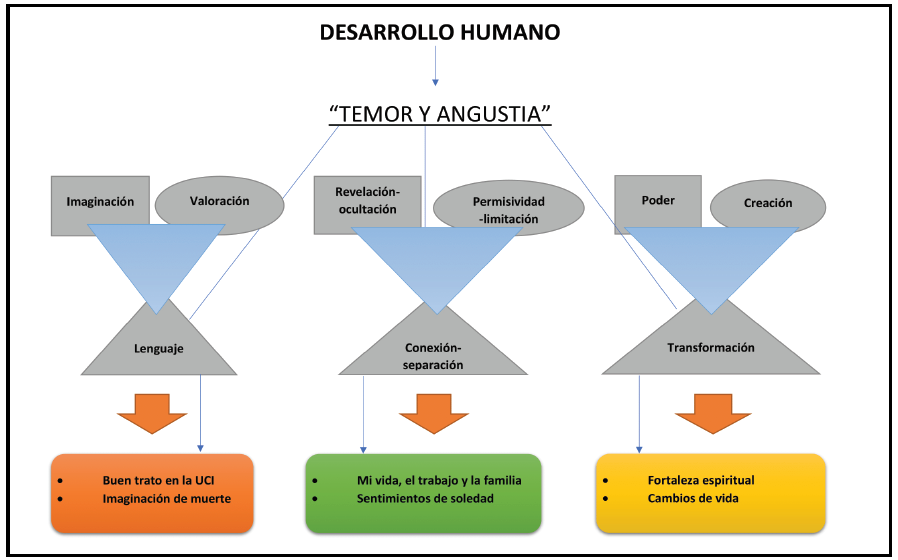 Figure 1: Topic and subtopic scheme in light of Rizzo's theory of human development.
Source: Researchers own elaboration
Figure 1: Topic and subtopic scheme in light of Rizzo's theory of human development.
Source: Researchers own elaboration
1.Theoretical principle: Imagination - Assessment - Language:
• Subtopic 1: Good treatment
The meanings that adults build through the experience formed by their language and imagination, allow them to build a limited reality that is expressed verbally through the values and reflections present in a situation, therefore, nursing as a pillar of care provides the inputs for the human being to illustrate, explore and interpret their experiences.
In this case, the care provided by the health personnel working in the ICU must convey confidence and security to communicate effectively with patients. Despite the limitations and emotional difficulties that individuals present during their hospitalization, for the adults who graduated from the ICU, the good treatment and care provided by the interdisciplinary team was essential.
Good care received in the ICU contributes to better patient outcomes, including a shorter stay, greater satisfaction, and better communication in decision-making. This care can also be indirectly where the patient, through technology, receives constant surveillance through monitoring and systematization. In this way, care is a fundamental part in the recovery of patients, since they feel more support and greater security during their stay in the ICU. The participants expressed the aspects related to good care during their stay, as follows:
PE1: "[...] they are more aware of one ... more monitored ... they take his vital signs every so often, they are aware of the drug than one thing, than the other [...]".
PE2: […] “I called them and they were there right away… they were all pending”.
PE6: ““the attention, that, that was quite good, it was good […], I have no complaints about all the staff [….]”.
PE8:“well, the service was very good […] it was super good, I'm not complaining”.
• Subtopic 2: Imagination of death.
Imagination as a principle of the theory of human development (12), establishes the vision that an individual has of reality, a vision of his personal and reflective knowledge taken from the meanings constructed in an unexpected situation, consequent on a health process.
In the report of the experience of the adults who graduated from the ICU, the perception of severity and risk of life was expressed with feelings of closeness to death, this being an experience of great impact.
In critically ill patients, the idea of death is manifested by feelings and fears of suffering. However, the participants also reported emotional reactions in which they experience imaginations of death, a feeling that is defined as a situation generated by a circumstance in which an individual finds himself at the time of being in danger. The participants report that:
PE3:"... they have always said whoever enters the ICU does not leave alive [...]"
PE8:[….] "It was very traumatic… When they mention ICU to one… it is… the worst, the worst condition […]"
PE9:“[…] I never thought I was hospitalized in the ICU… I thought about many things, I thought that I was not going to stop anymore, […] when one arrived at an ICU I ended up… dead […]”
Some hospitalized patients experience feelings of fear, uncertainties and anguish due to the serious and fatal events that occur during their hospital stay, which generates an alteration in the patient's environment, manifested in the following descriptor:
PE2:“[…] it's not pleasant at all… because one sees a lot of things there, others get complicated”.
PE8: "I saw when the patient in front died, I was scared, I said ... I too will go to die, of course one gets scared."
• 2. Theoretical principle: Revelation-Concealment, Connection-Separation, Permissiveness-Limitation:
• Subtopic 3: My life, work and family
Human beings in their daily life establish rhythmic guidelines that structure their experiences and experiences; In their environment, the adult graduated from the ICU builds patterns of relationships with others that cause freedoms or restrictions.
Therefore, the limitations presented by hospitalization generate feelings of frustration, due to the physical and emotional restrictions that the patient faces due to not being independent; thus, reluctance is forged in family, social and work aspects due to their illness, physical and / or emotional consequences.
PE3:“[…] I was working… I had to resign… because…. it's my life or work […] ”.
PE9:“[…] I had to stop working, because my illness prevented me… […].
Another important aspect that the participants revealed were the feelings of discouragement and fear, when thinking that they could not continue raising their loved ones, since they were the ones who supported the economy of their homes. They argue that
PE6:“[….] My family is what worries me the most… I have not finished raising or educating my children yet, […]”
PE8:"[...] I am a mother who is the head of the family ... imagine! I was bedridden ... and it was the one that generated the income."
•Subtopic 4: Feelings of loneliness
The family nucleus is considered one of the most important aspects for society, because it represents the main support network, incentive and source of strength. In this way, patients need family support for their transformation and emotional motivation. Thus, family isolation was considered a stressor that generates anguish.
Rizzo (12), points out that the connection and separation patterns create distancing ties between close people, that is, one is able to survive in the absence of a loved one, but always establishing connection ties.
In this context, the participants expressed feelings of loneliness during their stay in the ICU, referred to as moments in which they feel isolated from their loved ones and required their closeness as support in those difficult situations they faced:
PE1: "[...] one feels far away, just [...]".
PE9: “the first time it hit me because […] I had never been in a hospital alone”.
PE10:"... I felt alone, there were many relatives ... and they were not allowed to enter"
PE11:"some want to see their children, husband, all their relatives, but they would not let them in"
Restrictions on visits to the intensive care unit are part of institutional and regulatory policies that have been established since its inception, however, for some patients the company of their relatives is of utmost importance, and they express the need to feel support as an essential aspect when it comes to your recovery:
E1. I1: “así le toca a uno como paciente, todos los días estar jodiendo allá para que le puedan hacer las cosas” y E1. I3: “esto toca estar puyando allá porque si no, no lo llaman a uno”.
PE2:“[….] Lack of communication… with my family members,… I saw her only one hour a day”.
PE5:““[…] to receive a single hour of visit… one would like to be accompanied for more time […]”.
PE8:“[…] it is difficult not to receive visitors… I couldn't see my children”.
3. Theoretical principle Power - transformation - creation:
The experiences of facing a difficult situation, separating from loved ones and imagining being close to death, awakens in the individual feelings of change and transformation; changes that build infinite possibilities of being, how to be, and what to be, with whom to relate and how to transcend the visible-invisible becoming to become the emerging now, in this principle two subtopics are presented:
• Subtopic 5: Spiritual strength.
From a holistic point of view, patients must satisfy their spiritual needs, in that sense, they need their spirituality to maintain their inner strength, motivations and beliefs, being these sources of help. One aspect within the spiritual area is religious beliefs, where a large part of the patients cling to them, give their trust and help them in accepting the disease, being a source of hope.
Feelings of uncertainty are related to fear, time, and vulnerability due to ignorance of the unexpected future. Once the participants experience moments of loneliness due to their clinical situation, they feel the need to seek supreme support, to have inner tranquility and to know how to cope with moments of anguish and imaginations of death, so that the participants rely on God and increase their spiritual strength to get out of this situation, expressed like this:
PE1: "spiritually one is strengthened ... God ... is what strengthened me the most"
PE5: “[…], my illness invited me… to seek greater closeness with God… to have a spiritual growth […]” “[…] we all cling to God, […]”
PE8: "God ... is the one who gives us life, every day I clung to God, and asked him for my recovery [...]"
• Subtopic 6: Life changes
Changes are part of life, they are faced at some point by the individual, either by natural, social, moral or spiritual consequences, causing anguish and concerns in the human being.
When the human being discovers his changes, he modifies his understanding, that is, they change the patterns of life, the reality of the world and profoundly transform the visible being into the now emerging being
In this regard, the participants state that they feel a change as a result of the situation they experience in the ICU, there is an increase in the value of life, they are aware of the change measures they should take and they reflect on past situations and present situations. that favor change.
PE1: “[…] value… life more… if there are going to be changes in my life… it will no longer do the same […]”.
PE10: “[…] I will be closer to my family and I will lean on them”.
Likewise, the changes involve important modifications in the lifestyle, changes in the conduct and behaviors of the people, sometimes it is very difficult for them to adhere permanently to treatment and / or rehabilitation. Changes such as quitting smoking, starting physical activity, nutritional habits and in some cases modifying or stopping their work activities, usually generate feelings of frustration and helplessness in patients, but at the same time these changes generated by the stay for the UCI, leads them to reflect on the maintenance or recovery of their health, as well as the meaning of family.
PE3:“[…] it serves as an experience… taking more drastic measures… of eating habits […].
PE5:"[...] a situation that allows one to make a global analysis of what life has been ... to generate big changes ... make big analyzes to look at the many habits that will have to start [...]".
PE6: "one learns to love things more, his family, he misses his home ..."
Discussion
The results found in this study solve a felt need of researchers and nursing professionals where understanding the meaning of the experience of patients who once went through the intensive care unit will allow the entire interdisciplinary team to develop plans with the patients during their stay in the ICU, so that they have a satisfactory recovery process, which will improve their perception and the quality of the service.
It should be noted that the results found coincide with other investigations that have approached this phenomenon from the disciplinary point of view as an imminent and methodological concern with this individualistic approach. Regarding the demographic characteristics Beltrán (5), states in his research study that he included 9 adults between 24 and 80 years of age who were critically ill and hospitalized in the ICU. Similarly, Santiago and Vargas (26) interviewed nine patients between 59 and 74 years old who were hospitalized in a coronary intensive care unit with a diagnosis of acute myocardial infarction. Being consistent with the population group participating in this study.
The experience of the participants was described as “fear and anguish”, which are feelings generated by having contact with the intensive care unit, which is consistent with what is described by the authors Zambrano et al. (27), who state that feelings are an essential part of a person in daily life and when having to face a disease process, a series of concerns are generated in the individual that can interfere with their recovery. Anguish, suffering and instability are the feelings that are experienced in this situation.
Vasconelos et al. (28), in their research results, express that in some patients, especially in older adults, changes in family relationships are manifested mainly due to the fear of the appearance of a significant lack of independence that transforms the role of caregiver to that of careful subject.
On the other hand, Beltrán (5), concludes that patients describe the experience and the meaning of suffering, which was a component of the disease that contributed significantly to the harshness of the situation. The experience of critically ill patients in an ICU is very complex and full of contrasts. One of these contrasts is shown in the way the participants consider their experience, which ranges from "normal" and "incredible" to "harsh", "difficult", "sad" and "horrible" for the people who live it.
Regarding good treatment, the study participants expressed the importance of care by the staff working in the intensive care unit, Luiz, Caregnato and Costa (29), refer that humanized care in ICUs, make reference to the ability to provide care based on the needs of the other, appreciating even the slightest thing that bothers or perceives the patient as a threat, the constant accompaniment starts from the respect and consideration of that human being that requires the explanation of each activity to be done to reduce suffering and fear, as well as the family's perception of care.
Admission to the ICU generated feelings of fear in participants, where the feeling of death was the most manifested according to their social and cultural beliefs. This is highlighted by Zambrano et al. (27), who describe that these feelings are influenced by previous hospital experiences and by their cultural beliefs, such as fear of death. Similarly, Blanca et al (30) concluded that the patient has a fear of death when he feels it very close, ignorance of the consequences of the disease and everything that happens around him, and of an unforeseen future that completely changes his lifetime. For their part, Soares, Da Cunha and Biondo (31), in coherence with what has been described, also state that hospitalization in an ICU generates innumerable uncertainties and concerns, since it is an unknown environment that causes fear, mainly due to the association with death due to the clinical severity of hospitalized patients.
Regarding the subtopic My life, work and family, all the frustrations felt by the participants of not being able to continue with the activities and roles that they had been performing before entering the ICU and the changes generated by said hospitalization are taken into account. Indeed, the intervention may present various psychological alterations as a consequence of adaptation to the new situation, in which patients find themselves in a strange or unfamiliar environment, which deprives them of their usual interactions and sensations, while they are constantly assaulted by sensory stimuli strangers (32).
For this reason, it is considered that the environment of the ICU affects patients psychologically in a negative way. In addition, they have to abandon, at least temporarily, the roles they previously played (family, work, etc.) or even change them (27 - 33).
As for the feelings of loneliness, they were expressed by the participants regarding the need to have company from their family members and to feel constant support from them and thus be able to feel more calm during their hospitalization in the ICU.
In the same way, Beltrán (6), considers that the lonely environment is perceived by the patients in the ICU, it is the fact that the family company was subjected to a restrictive scheme and the control measures for the admission of people imposed by the administration hospital or by the health team. He adds that loneliness is due to the absence of those whose company is desired, to receive those words that patients want to hear, but cannot hear from the people who are important and meaningful to each one (2). Given this, Goularte, Gabarra, and Moré (34) express that professionals, in recognition of this, perceive the flexibility of the visit as beneficial for patients and their families in the ICU.
On the contrary Baharoon et al. (35), when measuring family satisfaction in critical care units, found that it is not influenced by the frequency of visits, despite reducing symptoms of depression and anxiety.
Spiritual strength was considered the most important tool that the participants found during their stay in the intensive care unit, since it strengthened them more with God. Collado (36) refers that spirituality is an intimate and transcendent phenomenon, a vital phenomenon for the development of the patient's health recovery. It is also considered a strength and a source of motivation and search for the meaning of life. This is why the spiritual care offered by the nursing staff must have a sense of responsibility, respect and dedication to the patient, especially if the patient is in the process of death. As expressed by Soto, Olivella and Bastidas (37), when nursing care interacts with the fragility and suffering of the patient and / or the family, it leads them to make spiritual care visible, based on respect for life and the dignity of person.
Finally, discharge from an intensive care unit goes hand in hand with medical indications and prescriptions, which will guide the patient on improving or maintaining health. Therefore, the study participants reflect on and analyze those modifications that they must have in their daily lives as a result of the illness for which they entered the ICU. Medina et al. (38), sustain that the diagnosis of chronic disease changes the way a person sees himself and his life; deeply affects your self-concept, because aging and changes in the psychological sphere make it difficult to adapt to the disease, your life project will have to be reviewed and often, you will not be able to know what its course will be. Likewise, Baeza and Quispe (39) reveal that post-intensive care syndrome (PICS) affects between 30% and 50% of patients after critical illness and is characterized by physical, neuropsychological or emotional symptoms such as anxiety, depression or post-traumatic stress; These problems begin to appear when the patient is in the ICU and may persist after discharge, their consequences impact the quality of life of patients and their families.
Finally, Díaz and Mercado (40) describe that people's behavior and coping models with the disease can play an important role in its course and in whether or not a patient complies with medical prescriptions. Those people who manage to adhere adequately to the behavioral regimes that each disease requires to achieve a good evolution will be able to achieve better control of the disease and increase or persevere in their quality of life; in addition to considering that health professionals carry out, together with sick people and their families, advance planning of care, since it has been reported that this benefits patients.
In general, the findings provide theoretical support to nursing research to identify the phenomena, which, although not measurable, can be understood, which will allow a global and holistic analysis of patients and the various circumstances that live due to some deterioration of their health is physical or psychological where the family is involved and contribute in a very creative way in solving identified problems.
Conclusions
•According to the findings, it is concluded that the stay of adult patients in the intensive care unit, triggered experiences and feelings generated by factors such as ignorance of the environment, social and cultural perceptions about death, in addition to changes such as learning to value to the family and take advantage of the time with her.
• By understanding the experience felt by the participants, it can be affirmed that for them the support of the family nucleus, the good treatment by the interdisciplinary team and learning the value of the family and the time lived is essential.
• The intensive care unit has visiting restrictions which are formal and institutional. This type of hospitalization, being different for them, generated the need to have their relatives close by in the recovery process; What in a certain way triggered in them, apart from fear and anguish, the feeling of loneliness due to feeling isolated and dependent on other people; thus seeking a greater spiritual consolidation and closeness to God.
• The good care by the interdisciplinary team of the ICU, managed to establish safety and tranquility in the patients during their stay, these actions allowed to minimize negative feelings, thus achieving a more satisfactory recovery in the hospitalization process, highlighting the importance of humanization of care.
•Lastly, the intensive care unit caused changes and transformations in the lives of the participants, many of them consequently due to their pathology, which affected some of the work and social roles they performed.
Conflict of Interest
The authors declare no conflict of interest.
Bibliographic References
1.Santiago de Castro E, Vargas-Rosero E. Experiencia de estar hospitalizado en una unidad de cuidado intensivo coronario de Barranquilla. Av. Enferm [Internet]. 2015 [Citado 04/09/17];33(3):381-390. Disponible en: http://www.scielo.org.co/pdf/aven/v33n3/v33n3a06.pdf
2.Soto del Arco F. Manual de ventilación mecánica para enfermería. 1ra ed. Editorial Médica Panamericana.; 2017.
3. Bohórquez A, Ramírez AC, Rodríguez EE, Polentino CV, Aceros MZ. Suspiro de vida: vivencias de los pacientes de la Unidad de Cuidados Intensivos sometidos a soporte ventilatorio. Rev. cienc. cuidad. [Internet]. 2016 [citado 16 de mayo de 2020];8(1):61-9. Disponible en: https://revistas.ufps.edu.co/index.php/cienciaycuidado/article/view/482
4. Amorós-Cerdá S, Arévalo-Rubert, MJ, Maqueda-Palau R, Pérez-Juan E. Percepción de la intimidad en pacientes hospitalizados en una Unidad de Cuidados Intensivos. Enf intensiva [Internet]. 2008 [ consultado 16 de octubre de 2018];19(4):1–11. Disponible en: https://dialnet.unirioja.es/servlet/articulo?codigo=2783407
5.Beltrán-Salazar O. La experiencia de estar hospitalizado en una unidad de cuidado intensivo. Rev. Aquichan [Internet]. 2009 [ consultado 30 de abril de 2018] ;9(1):1–9. Disponible en: https://aquichan.unisabana.edu.co/index.php/aquichan/article/view/167/1668
6.Beltrán-Salazar O. Estar críticamente enfermo significa no ser capaz y no poder decidir. Index Enferm [Internet]. 2008. [ consultado 30 de abril de 2018]; 17(2):92–96.
7. Prieto-Martínez P, Suárez Rodríguez N, Gómez Gómez L, Cárdenas Bolivar Y, Celis-Rodriguez É. Percepciones de dignidad y respeto en Unidades de Cuidado Intensivo. Acta Colombiana de Cuidado Intensivo. [Internet]. 2020 [consultado 16 de mayo de 2020]; 20(1):1–74. Disponible en: https://doi.org/10.1016/j.acci.2020.01.005
8.Mijangos-Fuentes K. El Paradigma Holístico de la Enfermería. Rev Salud y Adm. [Internet]. 2014 [consultado 9 de mayo de 2019]; 1(2):1–6. Disponible en: https://revista.unsis.edu.mx/index.php/saludyadmon/article/view/86
9. Peña-Ortiz LM, Hernández-Moncada YA, Morales-Morales JM, Zambrano-Plata G, Sánchez C. Life heartbeat: experiences of patients with cardiovascular disease in an intensive care unit. Rev. cienc. cuidad. [Internet]. 2019 [citado 14 de mayo de 2020]; 16(2):46-8. Disponible en: https://revistas.ufps.edu.co/index.php/cienciaycuidado/article/view/1607
10. Martínez-González L, Olvera-Villanueva G. El paradigma de la transformación en el actuar de enfermería. Rev Enferm IMSS [Internet]. 2011 [consultado 30 de abril de 2018]; 19(2):105–7. Disponible en: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=31760
11. Baeza-Gómez I, Quispe-Hoxsas L. Proyecto “Humanizando los Cuidados Intensivos”, nuevo paradigma de orientación de los Cuidados Intensivos. Rev. Bioética y Derecho [Internet]. 2020 [citado 2020 mayo 16]; (48):111-126. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1886-58872020000100008&lng=es
12. Alligood-Raile M. Desarrollo humano. In: Modelos y teorías en enfermería. OCTAVA. Barcelona España; 2015. p. 451–81.
13. Heidegger M. Ser y tiempo. Madrid: Trota; 2012.
14.Mendieta-Izquierdo G, Ramírez-Rodríguez J, Fuerte J. La fenomenología desde la perspectiva hermenéutica de Heidegger: una propuesta metodológica para la salud pública. Revista Facultad Nacional de Salud Pública: El escenario para la salud pública desde la ciencia [Internet]. 2015 [consultado 8 de septiembre de 2019]; 33(3):435-443. Disponible en: https://dialnet.unirioja.es/servlet/articulo?codigo=5214008
15. Muñoz-Pérez E. Trascendencia, mundo y libertad en el entorno de Ser y Tiempo de Martín Heidegger. Veritas [Internet]. 2015 [consultado 8 de septiembre de 2019]; 32:95-110. Disponible en: https://scielo.conicyt.cl/scielo.php?pid=S0718-92732015000100005&script=sci_arttext
16.Castillo-Espitia E. La fenomenología interpretativa como alternativa apropiada para estudiar los fenómenos humanos. Investigación y Educación en Enfermería [Internet]. 2000 [consultado 8 de septiembre de 2019]; 18(1):27-35. Disponible en: http://portal.amelica.org/ameli/jatsRepo/105218294002
17.Denzin NK, Lincoln S. Collecting an interpreting qualitative materials. London: Sage Publications.; 1998. p.179-210.
18.Creswell JW. Qualitative inquiry and research design: choosing among five traditions. London: Thousand Oaks, CA. Sage; 1997.
19.Starks H, Brown-Trinidad S. Choose your method: a comparison of phenomenology, discourse analysis, and grounded theory. Qualitative health research [Internet]. 2007 [consultado 16 de Octubre de 2018]; 17(10):1372-1380. Disponible en: https://pdfs.semanticscholar.org/a317/738b3a28d7c2c1af03fd1e22f67058342781.pdf
20.Lincoln YS, Guba EG. Naturalistic Inquiry. Estados Unidos: Age Publications.;1985.
21. Guba EG, Lincoln YS. Epistemological and methodological bases of naturalistic inquiry. Educ Tech Res Dev [Internet]. 1982 [consultado 16 de octubre de 2018]; 30(4):233-52. Disponible en: https://link.springer.com/article/10.1007/BF02765185
22.Bonilla-Castro E, Rodríguez-Sehk P. Más allá del dilema de los métodos: la investigación en ciencias sociales. Buenos Aires.: Editorial Norma.; 2005.
23.Critical Appraisal Skills Programme Español. Entendiendo la evidencia de estudios cualitativos 10 preguntas para ayudarte a entender un estudio cualitativo. [Internet]. 2016 [citado el 25 de mayo de 2019]. p. 1–6. Disponible en: http://www.redcaspe.org/herramientas/instrumentos
24.República de Colombia. Ministerio de la Protección Social. Resolución No. 8430, octubre 4, por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. [Internet]. Bogotá D.C.: Ministerio de la Protección Social; 1993 [consultado el 10 de noviembre de 2015]. Disponible en: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/RESOLUCION-8430-DE-1993.PDF
25.Pellegrini A, Macklin R. Investigación en Sujetos Humanos: Experiencia Internacional. Santiago de Chile: Programa Regional de Bioética OPS/OMS; 1999: 33-46.
26. Santiago-de-Castro E, Vargas-Rosero E. Experiencia de estar hospitalizado en una unidad de cuidado intensivo coronario de Barranquilla. Av.enferm. [Internet]. 2015 [Consultado 15 febrero 2018]; 33(3):381–90. Disponible en: http://bdigital.unal.edu.co/60480/1/41841-281572-1-PB.pdf
27.Zambrano-Plata G, Ferreira-Cardona J, Lindarte-Clavijo A, Niño-Bayona C, Ramírez-Rodríguez N, Rojas-Bautista L. Entre la incertidumbre y la esperanza: Percepciones y motivaciones de los pacientes hospitalizados en la unidad de cuidados intensivos (UCI). Rev. cienc. cuidad. [Internet]. 2016 [Consultado 15 Febrero 2018]; 7(1):52-60 Disponible en: http://revistas.ufps.edu.co/ojs/index.php/cienciaycuidado/article/view/493
28.Vasconelos EV, Freitas KO, Silva SED, Baia-RSM, Tavares RS, Araújo JS. O cotidiano de familiares de pacientes interna-dos na uti: um estudo com as representações sociais. Re-vista de Pesquisa Cuidado é Fundamental [Internet]. 2016 [acceso 16 may 2020]; 8(2):4313-4327. Disponível em: http://www.seer.unirio.br/index.php/cuidadofundamental/article/view/4366
29. Luiz FF, Caregnato RCA, Costa MR. Humanization in the Intensive Care: perception of family and healthcare professionals. Revista brasileira de enfermagem [Internet]. 2017 [acceso 16 may 2020]; 70(5):1040-1047. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pi-d=S0034-71672017000501040
30. Blanca-Gutiérrez JJ, Blanco-Alvariño A, Luque-Pérez M, Ramírez-Pérez M. Experiencias, Percepciones y Necesidades En La Uci: Revisión Sistemática De Estudios Cualitativos. Enferm glob. [Internet]. 2008 [Consultado 15 febrero 2018]; 12(1):1–14. Disponible en: https://revistas.um.es/eglobal/article/view/822/842
31. Chaves-Soares E, Pinheiro da Cunha JX, Santana-Biondo C, Lomanto-Rocha AK. Representação social de pacientes sobre a unidade de terapia intensiva. Revista Enfermagem Atual In Derme, [Internet]. 2020 [Consultado 6 Mayo de 2020]; 91(29):33-39 Disponible en: http://revistaenfermagematual.com/index.php/revista/article/view/531/602
32. Amengual G. El concepto de experiencia: de Kant a Hegel. Topicos [Internet]. 2007 [Consultado 15 febrero 2018]; 15:1–20. Disponible en: https://www.redalyc.org/pdf/288/28811907001.pdf
33.Cabrera-Saavedra J, Soledad-Rivera M, Jaman-Mewes P. Significados de la experiencia de una enfermera con su madre hospitalizada en una unidad intensiva coronaria. Revista Horizonte de Enfermería [En línea]. 2020 [Consultado 15 Mayo 2020]; 25(1):23-31. Disponible en:
34.Nunes-Goularte P, Macedo-Gabarra L, Ojeda-Ocampo CL. A visita em Unidade de Terapia Intensiva adulto: perspectiva da equipe multiprofissional. Rev. Psicol. Saúde [Internet]. 2020 Abr [Consultado 6 Mayo de 2020]; 12(1): 157-170. Disponible en: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S2177-093X2020000100012&lng=pt
35.Baharoon S, Al-Yafi W, Al-Qurashi A. Al-Jahdali H, Tamim H, Alsafi E, Al-Sayyari AA. Family Satisfaction in Critical Care Units: Does an Open Visiting Hours Policy Have an Impact?, Journal of Patient Safety. [Internet]. 2017 [Consultado 16 Mayo de 2020]; 13(3): 169-174. Disponible en: https://www.doi.org/10.1097/PTS.0000000000000140
36.Collado R. Cuidado espiritual, labor del profesional de Enfermería. Rev 360 [Internet]. 2010 [Consultado 2 dic 2018]; 5:1-3 Disponible en: http://cremc.ponce.inter.edu/360/revista360/ciencia/Cuidado%20espiritual%20enfermeria.pdf
37.Soto-Morales AM, Olivella-Fernandez MC, Bastidas-Sanchez CV. Cuidado espiritual al adulto mayor, elemento del conocimiento y práctica de enfermería. Rev. cienc. cuidad. [Internet]. 2020 [citado 16 de mayo de 2020]; 17(1):123-31. Disponible en: https://revistas.ufps.edu.co/index.php/cienciaycuidado/article/view/1563
38.Medina-Fernández I, Polanco-Tinal P, Tello-García M, Esparza-González S. Propuesta de cuidados de enfermería en la adaptación de autoconcepto de adultos mayores con diabetes tipo 2. Revista Española de Enfermería de Salud Mental [Internet]. 2019 [Consultado 9 septiembre de 2019]; 6:27-32. Disponible en: http://www.reesme.com/index.php/REESM-AEESME/article/view/28/36
39. Baeza-Gómez I, Quispe Hoxsas L. Proyecto “Humanizando los Cuidados Intensivos”, nueKeydisvo paradigma de orientación de los Cuidados Intensivos. Revista de Bioética y Derecho, [Internet]. 2020. [Consultado 7 Mayo de 2020] 48:111-126. Disponible en: https://revistes.ub.edu/index.php/RBD/article/view/29173
40. Díaz-Medina BA, Mercado-Martínez FJ. Obstáculos y estrategias de afrontamiento en la atención renal: estudio cualitativo en jóvenes con enfermedad renal crónica en diálisis peritoneal. Saude soc. [Internet]. 2019 [Consultado 9 septiembre de 2019]; 28(1):275-286. Disponible en: https://www.scielosp.org/pdf/sausoc/2019.v28n1/275-286/es
Para citar este artículo / To reference this article / Para citar este artigo/
Ruidiaz-Gómez KS, Fernández-Aragón S. Fear and anguish: the patient's experience in the intensive care unit. Rev. cienc. cuidad. 2020; 17(3):7-19. https://doi.org/10.22463/17949831.1695